| Feature | Roux-en-Y Gastric Bypass (RYGB) | One Anastomosis Gastric Bypass (OAGB) | Notes |
|---|---|---|---|
| Image |
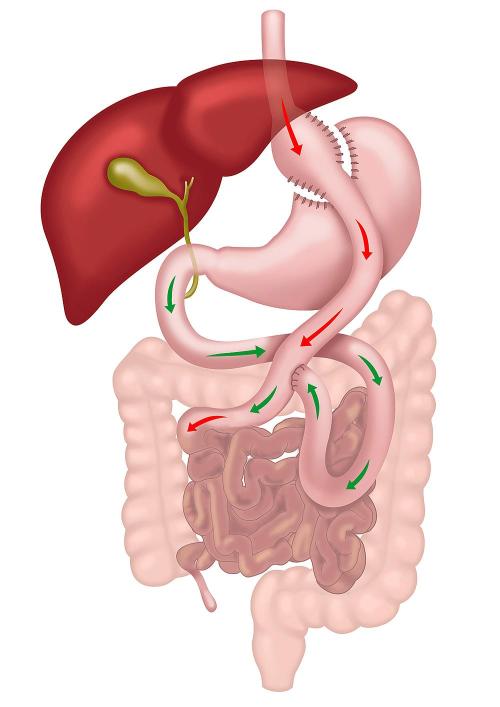
Roux-en-Y Gastric Bypass (RYGB) |
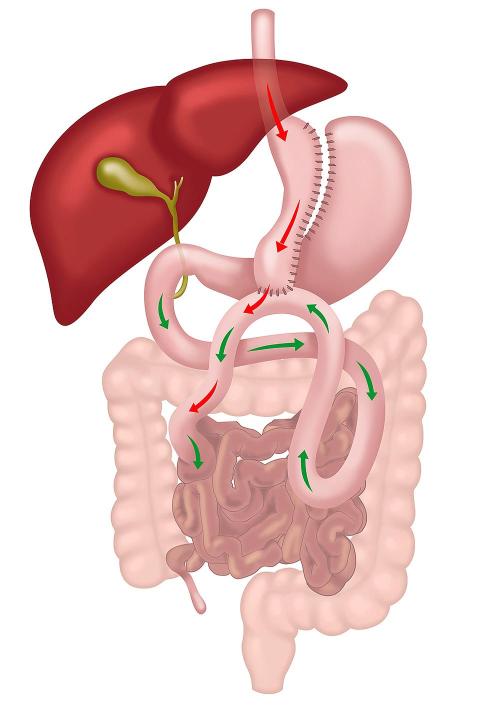
One Anastomosis Gastric Bypass (OAGB) |
|
| Mechanism of Action | Restricts food intake and reroutes small bowel to bypass absorption sites. | Restricts food intake with a single connection bypassing absorption sites. | Both induce hormonal changes (e.g., increased GLP-1, reduced ghrelin), improving satiety and glucose metabolism. |
| Stomach Modification | Small and narrow gastric pouch created (~30 mL). | Long narrow gastric pouch created (~150 mL). | OAGB pouch is longer compared to RYGB. |
| Number of Anastomoses | Two (gastrojejunal and jejunojejunal). | One (gastrointestinal). | The single anastomosis in OAGB simplifies the procedure and reduces operative time. |
| Bile Reflux | Rare. | Possible due to single anastomosis. | Bile reflux is a significant consideration in OAGB and may require revision surgery in symptomatic cases. |
| Risk of Marginal Ulcers | Small. | Small but likely higher than RYGB due to bile and acid exposure at the single anastomosis. | In both operations, the risk of marginal ulcers is higher in smokers or with use of NSAIDs (anti-inflammatory drugs). |
| Weight Loss Outcomes | 70–80% excess weight loss (EWL) or 30–40% of total body weight. | 70–80% excess weight loss (EWL) or 30–40% of total body weight. | Comparable weight loss outcomes in the first 2 years; durability varies depending on individual factors and compliance with lifestyle changes. |
| Improvement in Metabolic Conditions | Significant improvement in type II diabetes, insulin resistance, and metabolic syndrome. | Significant improvement in type II diabetes, insulin resistance, and metabolic syndrome. | Both procedures improve glucose homeostasis through hormonal changes and weight loss, often leading to remission of type II diabetes. |
| Risk of Internal Hernias | Higher due to two mesenteric defects. | Lower due to one mesenteric defect. | RYGB has a higher risk of hernias requiring surgical intervention. |
| Risk of Gastroesophageal Reflux Disease (GERD) | Reduced in most patients. | Bile reflux may mimic or worsen GERD symptoms. | Both can improve GERD, but OAGB's bile reflux risk can be problematic for some patients. |
| Suitability for NSAIDs | Contraindicated. | Contraindicated. | NSAID use is not advised in either procedure due to the increased risk of marginal ulcers. |
| Revisional Surgery Risk | Moderate. | Moderate. | Both procedures can require revisions for complications such as reflux, malnutrition, or inadequate weight loss. |
Join Our Weight Loss Surgery Seminar
Interested in taking control of your health and well-being? Join our free seminar to learn about weight loss surgery options and how they can change your life.
Next Seminar Date
Our next seminar will take place on:
Time: 6:00 PM – 7:30 PM
Location: The George Centre, Gregory Hills

Compare Bariatric Operations
Discover the differences between various obesity surgery options, from effectiveness to recovery times, in this comprehensive guide. Learn which procedure might be best suited to your health needs and lifestyle.

Frequently Asked Questions about Gastric Sleeve
Get answers to common questions about sleeve gastrectomy, covering everything from procedure details to expected outcomes. Understand what to expect and how this surgery could support your weight loss journey.

Frequently Asked Questions About Gastric Bypass
Explore key insights into the Roux-en-Y gastric bypass, including how it works and what to expect post-surgery. This FAQ guide addresses common questions to help you make an informed decision about your weight loss options.

Join Our Bariatric Support Group
Our support group is dedicated to supporting those on their bariatric surgery journey. Gain insights, share experiences, and find encouragement to help you achieve your health and weight loss goals.

Why Grazing is Bad
Understand why grazing can hinder weight loss and affect your bariatric surgery outcomes. This guide explains the impact of frequent snacking and offers strategies to maintain healthy eating habits.

Why Roux en Y Gastric Bypass Improves Heartburn
Learn how the Roux-en-Y gastric bypass can effectively reduce acid reflux symptoms. This article explains the mechanisms behind the surgery’s success in alleviating gastroesophageal reflux disease (GORD).

Pre-Op Diet Class
Prepare for bariatric surgery with our pre-op diet class, designed to guide you on essential dietary changes for a successful surgery and recovery. Learn key strategies to optimize your health and support your weight loss journey.

Our Technique for Gastric Sleeve
Explore each step of the sleeve gastrectomy procedure to understand how this effective weight loss surgery is performed. This guide walks you through the surgical process, from preparation to the final stages of the operation.

What is the Best Weight Loss Operation?
Choosing the right bariatric surgery can be life-changing, but with so many options, how do you decide? This article helps you understand which procedure might be best for you, based on your unique needs and goals.

FAQs about Hair Loss After Weightloss Surgery
Learn why hair loss happens after bariatric surgery and how to prevent and manage it

Are Your Weight Loss Goals Realistic?
Wondering how much weight you'll really lose after bariatric surgery? This practical guide helps you test your expectations with a simple weight loss calculator and goal-setting exercise. Discover what’s realistic, what’s not, and how to set yourself up for long-term success.
HOT
Bariatric Support Group
Connect with others on the same journey. Our support group offers guidance, motivation, and expert advice for long-term weight loss success.
Next Meeting: Monday 15th September 2025
Time: 6:00 PM – 7:30 PM
Location: The George Centre, Gregory Hills
Join NowAddress
Southwest Bariatrics
Suite 13, 42 Parkside Cres, Campbelltown NSW 2560
Suite 14, The George Centre, 1A-1B The Hermitage Way, Gledswood Hills, NSW 2557
surgery@southwestsurgery.com.au
Mo-Fr: 9:00 am to 5:00 pm